Prevalence and associations of nephrocalcinosis in pediatric kidney transplant recipients
Yaritzy Astudillo1, Debora Matossian1, Carlos Becerril-Romero1, Priya Verghese1, Stella Kilduff1.
1Pediatric Nephrology, Ann & Robert H. Lurie Children’s Hospital of Chicago, Chicago, IL, United States
Introduction: Nephrocalcinosis (NC) is common in kidney transplant recipients (KTRs) and linked to poor graft function in adults. The risks and causes in pediatric KTRs remain poorly described. This study aims to examine the prevalence and associations of nephrocalcinosis in pediatric KTRs.
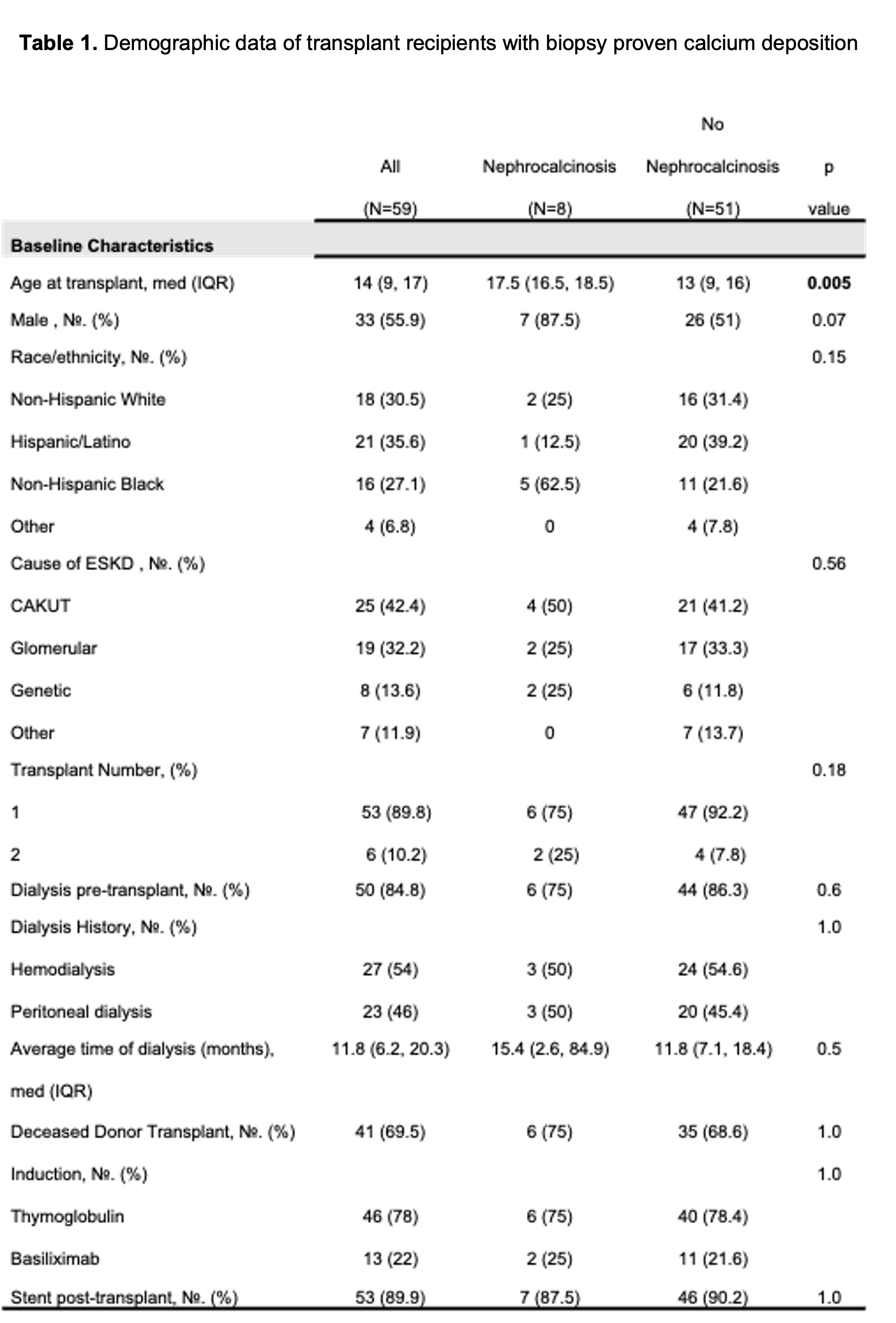
Methods: We analyzed pediatric KTRs <21 years of age who received a KT at a single center from 1/1/23-12/31/24 excluding multi-organ transplants. Descriptive statistics reported baseline characteristics, lab, and biopsy data by NC status, defined as having calcium deposits on kidney biopsy.
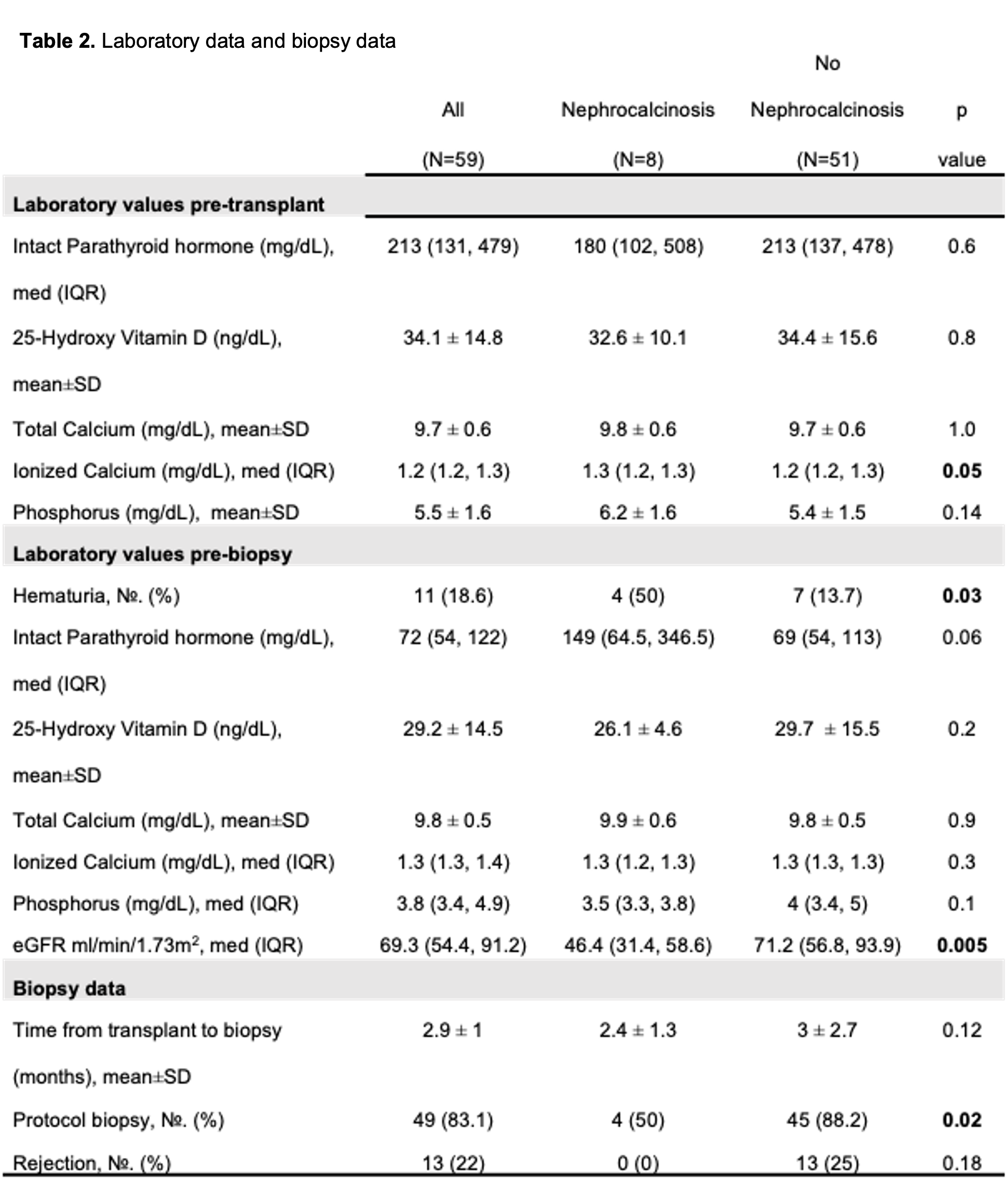
Results: 8 out of 59 KTRs had NC (13%) with median time to biopsy of 2.4±1.3 months (Table 1). KTRs with NC were older at time of transplant (median age 17.5 vs 13 years, p<0.005) and the majority were Black (62.5%) and male (87.5%). Median pre-transplant ionized calcium was 1.3 mg/dL in KTRs with NC vs.1.2 mg/dL without NC (p=0.05) (Table 2). Although not statistically significant, median pre-biopsy intact parathyroid hormone (iPTH) was higher among KTRs with NC (149 vs. 69 pg/ml; p=0.06). Median glomerular filtration rate (GFR) pre-biopsy in those with NC was lower at 46.4 vs. 71.2 mL/min/1.73m2 in those without NC (p=0.005). In KTRs with NC, 50% had hematuria on pre-biopsy urinalysis compared to only 13.7% in the non-NC cohort (p=0.03). Protocol biopsies were more common in recipients without NC (88.2% vs 50%; p=0.02). Despite a higher proportion of for cause biopsies (compared to protocol) in the NC cohort, no rejection was observed.
Conclusion: NC was commonly observed during the first-year post KT and was associated with a lower GFR and hematuria. In addition, recipients with NC were older and more likely to receive a biopsy for cause. Our NC cohort showed significant graft dysfunction, suggesting calcium deposition may be a key factor. Larger studies are needed to explore potential risk factors and the impact of NC on long-term KT outcomes.
[1] Pediatric Kidney Transplant
[2] Nephrocalcinosis
[3] Transplant Outcome
[4] Graft Dysfunction
[5] Mineral Metabolism