Long term outcomes of sirolimus based immunosuppression among haplotyped-matched pediatric living donor kidney transplant recipients
Adrian Banerji1, Alexis Gomez1, JoAnn Morey1, Isa Ashoor1, Nancy Rodig1.
1Division of Nephrology, Boston Children's Hospital, Boston, United States
Purpose: To examine long term outcomes of steroid and CNI sparing immunosuppression (IS) with sirolimus (SRL) following alemtuzumab induction amongst pediatric recipients of haplotype matched living donor kidney transplant (HMKT) compared to those receiving CNI based IS after either deceased donor kidney transplant (DDKT) or non-haplotype matched living donor kidney transplant (NHMKT).
Methods: Retrospective review of all kidney transplants at our center from 1/2017 to 12/2021. Patients with prior transplants, steroid based IS, or immediate surgical allograft complications were excluded. All received alemtuzumab induction and steroid sparing IS with mycophenolate mofetil (MMF) and tacrolimus (TAC). HMKT recipients were transitioned from TAC to SRL by 3 months. Patients were grouped by IS and donor type: SRL-HMKT, CNI-NHMKT, CNI-DDKT. Outcome measures of allograft rejection, failure, donor specific antibody (DSA) positivity, eGFR were collected over 3 years. Summary statistics were analyzed. Chi square test was used to compare binary outcomes.
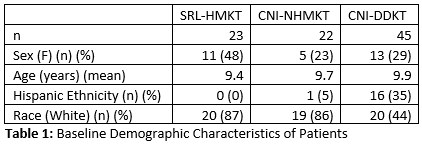
Results: 90 patients were included. Baseline age was similar between cohorts but SRL patients were more likely to be white and female than CNI patients (Table 1).
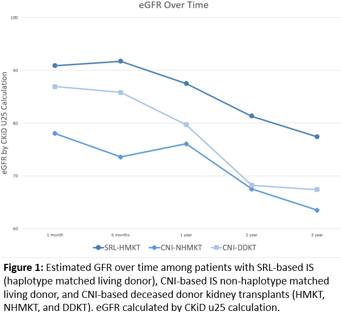
Three HMKT patients were never transitioned from TAC to SRL, two due to DSA+, one for parental preference. At 3 years, 16 patients remained on SRL. There were fewer episodes of acute rejection in SRL group (4% vs. 9% in CNI-NHMKT and 20% in CNI-DDKT), and less DSA positivity at 3 years (22% vs. 36% in CNI-NHMKT and 40% in CNI-DDKT). After exclusion of 3 HMKT patients who never received SRL, SRL patients had less DSA than CNI patients, 15% vs. 39%, p = 0.04. Graft survival among SRL recipients was 100% at 3 years, compared to 95% in CNI-NHMKT and 89% in CNI-DDKT. SRL group had higher eGFR at each time point (Figure 1). There was a single episode of mortality due to COVID infection in the CNI-DDKT cohort.
Conclusions: A CNI and steroid sparing IS protocol with alemtuzumab induction and early conversion to SRL in living donor recipients of haplotype matched kidney transplant shows acceptable allograft function and non-inferior rates of acute rejection, DSA positivity, and graft failure relative to CNI-based IS. Larger studies with longer follow-up are needed to confirm those findings.
[1] Pediatric
[2] Kidney
[3] Sirolimus
[4] Immunosuppression