Long-term follow up for pediatric kidney transplant recipients receiving IVIG for polyoma BK viremia
Jessica L Brennan1, Paul Brakeman2.
1Department of Surgery, Division of Transplant, UCSF Medical Center, San Francisco, CA, United States; 2Department of Pediatrics, UCSF Medical Center, San Francisco, CA, United States
Introduction: Polyoma BK virus (BKV) is a significant infectious complication in kidney transplantation leading to renal dysfunction and graft loss in up to 10% of kidney transplant recipients. Rates of BK viruria and viremia among kidney transplant recipients are noted to be 35-40% and 11-13% respectively. . Anti-viral and other therapies have proven ineffective. Careful reduction of immunosuppression is the mainstay of treating BK viremia and nephropathy; however, patients are at high risk for rejection during periods of reduced immunosuppression. Our goal was to evaluate the early use of intravenous human immunoglobulin (IVIG) combined with immunosuppression reduction to reduce the risk of rejection during active BK viremia.
Methods: We report on a series of ten pediatric kidney transplant patients ages 2-20 years who received IVIG in addition to immunosuppression reduction during the period 2017-2025. Seven of ten patients developed severe BK viremia during the first 9 months post-transplantation. IVIG was given at a dose of 0.67-1 gm/kg monthly. Baseline immunosuppression consisted of tacrolimus, mycophenolate mofetil (MMF) +/- prednisone, and MMF dose was reduced 50-100% depending on assessed risk for rejection and severity of BK viremia.
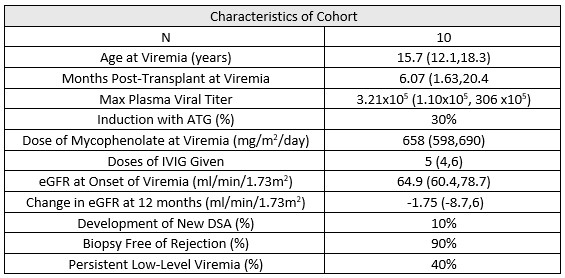
Results: In our cohort, all were primary transplants, 70% were deceased donor transplants, and 40% were pre-emptive transplants. BK viremia developed at a median of six months post-transplant with median max viral titers of 3.21x10e6 (see table 1). The median dose of mycophenolate at the time of viremia was 658mg/m2. The average number of IVIG doses was 5, using a dose range of 0.67-1 gram/kg. Three of the ten patients were converted to sirolimus after developing BK viremia with one patient continuing on sirolimus long-term. Persistent low-level viremia was defined as lasting for > 6 months and was seen in 40% of the cohort. Both patient and graft survival at one and three-year post treatment were 100%. Only one patient developed rejection.
Conclusion: Thoughtful immunosuppression remains the most important intervention to control BK viremia. Early initiation of IVIG infusions along with reduction of immunosuppression therapy in pediatric patients with severe BK led to clearance of BK viremia with a low rate of rejection and excellent 1 and 3-year graft survival. Prolonged periods of low-level BK viremia after IVIG did not affect long-term allograft outcomes.
[1] BK virus, pediatric kidney transplant
[2] BK viremia, IVIG