The role of the fungal biomarker Beta-D-Glucan (BDG) in diagnosing and guiding antifungal prescribing for fungal infections in paediatric liver and multivisceral transplant recipients
Sharath Manya1, Anil Dhawan1, Anita Verma2.
1Paediatric Liver, Gastroenterology and Nutrition Centre, King’s College Hospital NHS Trust, London , United Kingdom; 2Department of Infectious Sciences, King’s College Hospital, London, United Kingdom
Introduction: The risk of fungal infections (FI) in complex pediatric liver transplant recipients (PLTR) increases significantly because of cumulative exposure to various risk factors including increased length of hospital stay (LOHS), intensive care unit (ICU) stay, invasive plastic devices and prolonged antibiotics usage. Early diagnosis and prompt targeted antifungal therapy is key to improved outcomes.
We aimed to evaluate the potential role of BDG in diagnosing and prescribing antifungals in PLTR and multivisceral transplant recipients.
Methods: Fungal biomarker 1,3-β-D-glucan (BDG) was done in 254 patients over 18 month period for high risk patients admitted to the paediatric ICU and liver ward at King’s College Hospital. Ninety-six (37%) children with paediatric liver transplant (PLTR) and multivisceral transplantation (MVSTX) underwent systematic weekly BDG testing. A cutoff of >80 pg/ml in ≥2 samples prompted further testing for fungal infections (FI) via imaging, culture, or histology.
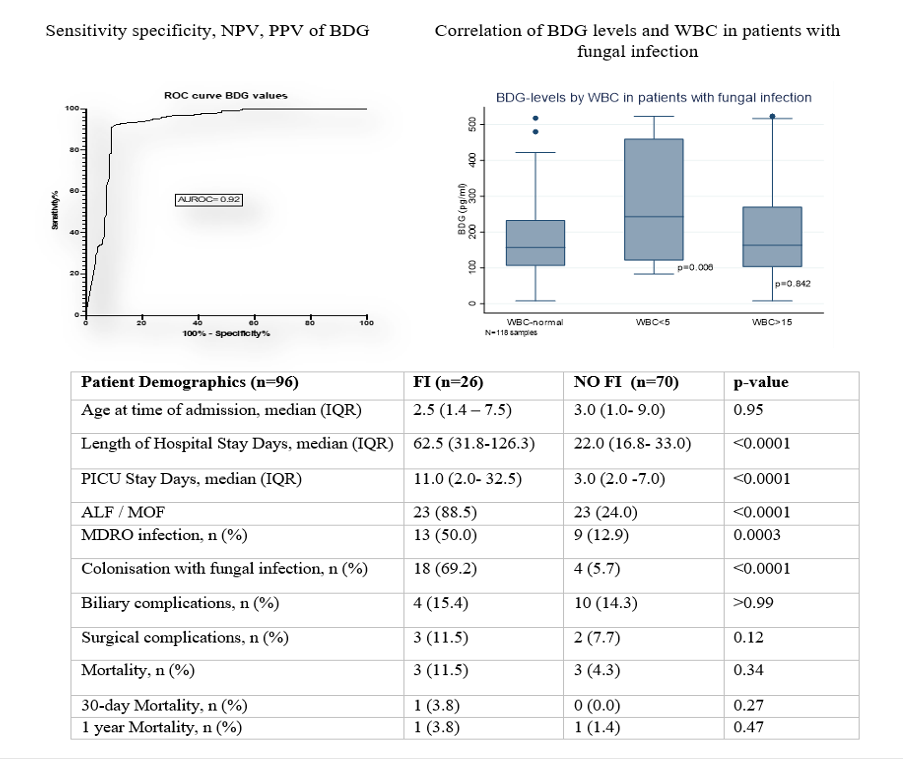
Results: 48/96 (48%) had ≥2 positive BDG samples and 25/96 (26%) were diagnosed with FI; only one case of FI had negative BDG. Sensitivity and specificity were 94% and 92% respectively, with a negative predictive value (NPV) of 96%. Negative BDG (80 pg/ml) safe guided antifungal cessation in >80% of cases, reducing treatment duration and cost. The patients with decreasing trend of BDG levels received a shorter duration of antifungals. Leucopenia was associated with an increased BDG and had longer duration of antifungals (Table).
Candida albicans represented 50% of infections (13/26), while non-Candida yeast (e.g. Geotrichum capitatum, Mucor circinelloides) accounted for 19% (5/26), all had positive BDG. The FI rates were higher in children who were transplanted for acute liver or multiorgan failure compared to chronic liver or intestinal failure. Ninety-days all cause mortality was 4%; no child died from FI, but children with FI had significant higher hospital and PICU stays.
Conclusion: Two or more than 2 positive BDG values of >80pg/ml has good diagnostic accuracy for FI in children with LT and MVST. The non invasiveness and high NPV makes BDG a potential biomarker to include in diagnostic algorithm for FI in targeted PLT and MVST patient populations.
[1] Liver Transplant
[2] Multivisceral transplant
[3] Fungal Infections
[4] Beta D Glucan
[5] Biomarker
[6] Antifungal